- — Corticosteroid (steroid) injections act like a 'fire extinguisher,' providing rapid but temporary anti-inflammatory relief without repairing damaged tissues.
- — Repeated cortisone shots carry a chondrotoxic threat, actively degrading joint cartilage cells, accelerating osteoarthritis, and weakening tendons over time.
- — Platelet-Rich Plasma (PRP) delivers concentrated autologous growth factors directly to joint defects, stimulating local tissue repair and providing superior long-term pain relief.
- — Clinical studies show that PRP is superior to corticosteroids for sustained pain relief and functional improvement at 6 and 12 months.
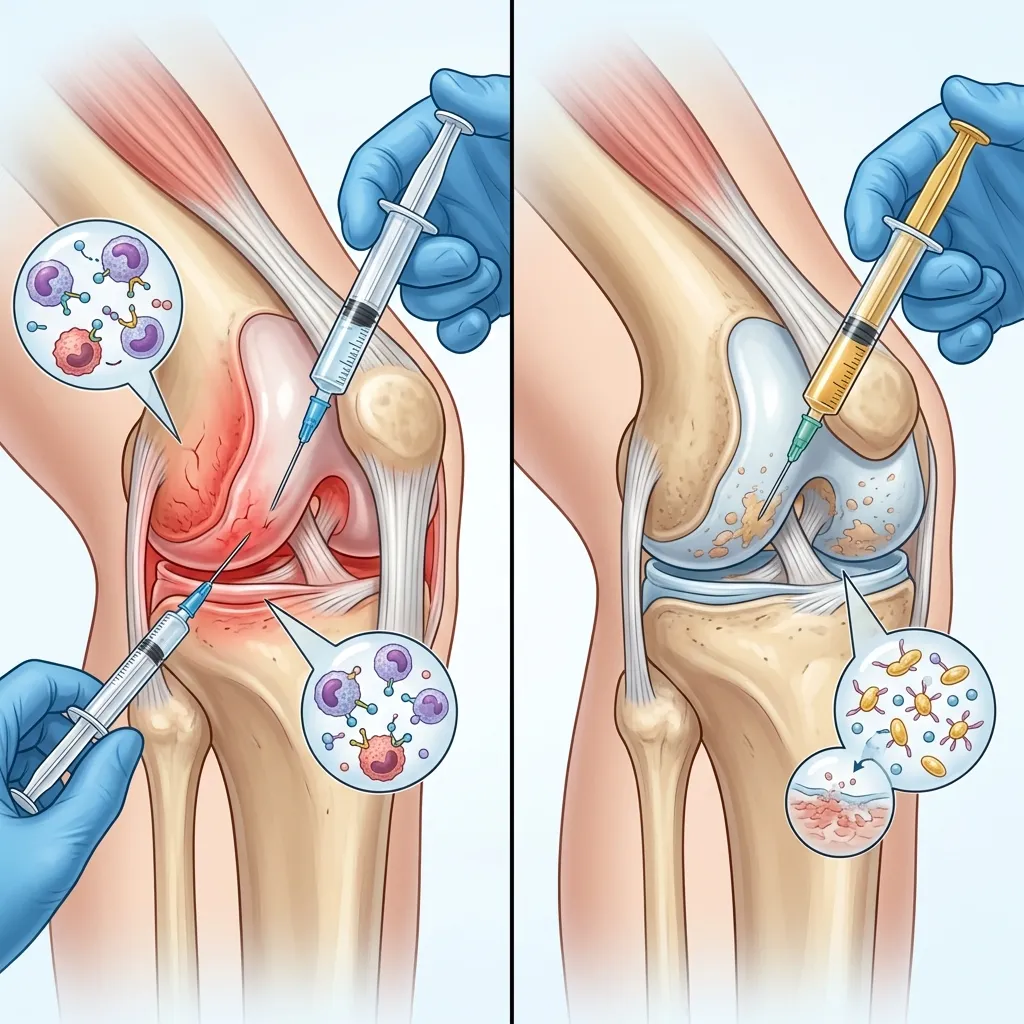
In my practice as a Physical Medicine and Rehabilitation (PM&R) specialist in Vigan, Ilocos Sur, I frequently consult with patients who are trapped in a frustrating clinical cycle. Typically, they present with chronic knee, shoulder, or hip pain that was initially treated elsewhere with a cortisone injection. They report that the first shot worked like magic, providing near-instantaneous relief. However, the second shot lasted only a fraction of the time, and by the third or fourth injection, the pain returned faster and significantly worse than before. This scenario is a classic manifestation of the limitations of synthetic anti-inflammatory therapies. To help patients understand their options, I often use a simple clinical analogy: the difference between a steroid injection and regenerative Platelet-Rich Plasma (PRP) is the difference between a fire extinguisher and a fertilizer.
When reviewing patient discussions and posts on online communities like Reddit threads, YouTube comments, and health forums (such as Inspire and PatientsLikeMe), a common pattern of anxiety emerges. Patients frequently share stories of getting temporary relief from cortisone only to experience worsening joint pain, asking if there is a safer, more permanent alternative. This patient voice highlights the need for honest education regarding orthobiologics. When a joint is highly inflamed, swollen, and hot, it is in a state of chemical crisis. In this acute phase, a steroid injection acts as a powerful fire extinguisher. It rapidly smothers the chemical fire of inflammation, quietening pain pathways. However, a fire extinguisher does not rebuild the burned walls of a house; it merely stops the immediate destruction. Once the chemical effect wears off, the underlying structural damage—the frayed ligaments, the thinned cartilage, and the unstable joint mechanics—remains. In contrast, regenerative Platelet-Rich Plasma (PRP) acts as a biological fertilizer. Instead of suppressing the body's processes, it stimulates a targeted, localized healing response. It delivers the necessary nutrients and cellular growth factors directly to the damaged tissues to encourage the body to lay down new collagen, preserve cartilage, and structurally stabilize the joint.
The Chondrotoxic Threat: How Repeated Cortisone Shots Degrade Your Joints
To understand why pain returns worse after repeated steroid treatments, we must look at the cellular impact of cortisone on joint tissues. A corticosteroid is a synthetic anti-inflammatory medication designed to mimic cortisol, a hormone naturally produced by the adrenal glands, to suppress immune activation and reduce swelling. While highly effective at reducing the cellular signals of inflammation in the short term, repeated exposure to high concentrations of corticosteroids is deeply detrimental to the long-term health of articular structures. This phenomenon is known as chondrotoxicity. In clinical terms, chondrotoxicity refers to the toxic degradation of cartilage cells (chondrocytes) and tendon cells (tenocytes) caused by exposure to certain chemical agents, including local anesthetics and corticosteroids.
Cartilage cells, or chondrocytes, are the only cells present in articular cartilage. They are responsible for producing and maintaining the extracellular matrix, which consists of collagen and proteoglycans that give cartilage its shock-absorbing capacity. Because cartilage is avascular—meaning it has no direct blood supply—it has an extremely limited capacity for self-repair. When a corticosteroid is injected into the joint recess, it suppresses the chondrocytes' ability to synthesize new collagen and proteoglycans. Furthermore, it directly induces chondrocyte apoptosis (cell death). As chondrocytes die, the cartilage matrix thins, softens, and becomes increasingly vulnerable to mechanical wear-and-tear.
This cellular damage has been clearly documented in high-level clinical trials. In a landmark randomized clinical trial published in the Journal of the American Medical Association, researchers evaluated the long-term effects of repeated steroid injections (McAlindon et al., 2017; PMID: 28510679). The study compared patients with symptomatic knee osteoarthritis who received intra-articular injections of triamcinolone acetonide (a common corticosteroid) every 3 months for 2 years against a control group receiving saline placebo injections. The results were stark: the patients treated with repeated corticosteroid injections experienced significantly greater cartilage volume loss compared to the saline group (a mean cartilage thickness loss of -0.21 mm versus -0.10 mm). More importantly, there was no significant difference in knee pain scores between the two groups over the 2-year period. This landmark study proved that repeated steroid shots degrade the joint structurally without providing any long-term pain management benefit.
The damage is not limited to cartilage. Tendons and ligaments are also highly vulnerable. When steroids are injected near or into tendon fibers, they inhibit fibroblast proliferation and collagen synthesis. This process impairs the mechanical integrity of the tissue, making it brittle. Over time, this degradation increases the risk of structural failure. Clinical literature has long established a clear link between local corticosteroid injections and subsequent tendon ruptures, particularly in the Achilles tendon and the rotator cuff (Tendon Ruptures Associated With Corticosteroid Therapy; PMID: 919538). When a patient presents to my clinic with a chronic tendon injury, I must carefully weigh the immediate anti-inflammatory benefits of a steroid shot against the very real risk of permanent structural weakening.
Patients experiencing this structural deterioration describe a wide spectrum of symptoms. They often report a sharp, stabbing pain when attempting to bear weight or rotate the joint, which frequently transitions into a persistent dull, deep ache during periods of rest. In many cases, the pain is not localized but rather behaves as a radiating discomfort that spreads down the arm or leg. In the mornings, they find that the joint feels incredibly stiff, requiring up to an hour of gentle movement to loosen up. They complain of a heavy, dragging sensation in the limb, feeling weak and unstable when performing daily activities like climbing stairs or carrying groceries. Some describe a tingling or burning sensation around the joint capsule, accompanied by mechanical catching or locking of the joint, and a prominent grinding sensation during active movement—a sign that the protective cartilage has thinned to the point of bone-on-bone friction.
Understanding Key Diagnostic and Clinical Terms
To help patients understand the physiological changes happening in their joints, it is helpful to establish clear definitions for several key medical terms that appear throughout this guide:
- An effusion is an abnormal accumulation of inflammatory fluid within a joint cavity or anatomical space, commonly occurring as a response to trauma, infection, or chronic arthritis (rayuma).
- An ultrasound refers to a non-invasive diagnostic imaging modality that uses high-frequency sound waves to visualize soft tissues, tendons, ligaments, and joints in active motion.
- An mri is a static diagnostic imaging technique that utilizes strong magnetic fields and radio waves to generate detailed, cross-sectional pictures of internal anatomy.
- A sprain means an injury to a joint ligament caused by sudden stretching or tearing of its fibers, often resulting in joint laxity and micro-instability.
- A tear occurs when the structural fibers of a muscle, tendon, or ligament are physically severed, leading to mechanical weakness and functional limitation.
Platelet-Rich Plasma (PRP): Concentrated Growth Factors for Active Tissue Repair
While steroid injections focus on chemical suppression of symptoms, Platelet-Rich Plasma (PRP) takes a direct biological approach by supplying the joint with a highly concentrated dose of active healing elements. Mechanically, Platelet-rich plasma (PRP) is an autologous blood concentrate that contains a high concentration of platelets, growth factors, and bioactive proteins prepared from the patient's own blood through centrifugation to accelerate tissue repair and regulate joint inflammation.
The process begins with a standard blood draw (venipuncture) in our clinic. The blood is collected in specialized sterile tubes and placed into a centrifuge, which spins the blood at high speeds to separate its components based on density. We extract the middle layer—the "buffy coat"—which contains the concentrated platelets, while filtering out the pro-inflammatory red blood cells. Platelets contain tiny storage sacs called alpha-granules. When injected into a damaged joint, these platelets become activated and release a massive cascade of growth factors, including Platelet-Derived Growth Factor (PDGF), Transforming Growth Factor-Beta (TGF-β), Vascular Endothelial Growth Factor (VEGF), and Fibroblast Growth Factor (FGF).
These growth factors act as biological keys that unlock cellular repair. They bind to receptors on the surface of local chondrocytes, stem cells, and synovial cells, directing them to:
- Downregulate inflammatory cytokines (like IL-1β and TNF-α) that degrade the cartilage matrix.
- Stimulate chondrocytes to produce new collagen and hyaluronic acid.
- Promote angiogenesis (the growth of new micro-capillaries) to deliver nutrients to the avascular joint space.
Recent high-level clinical evidence supports this regenerative mechanism. A comprehensive systematic review and network meta-analysis evaluated the comparative efficacy of various intra-articular injections for knee osteoarthritis (Diaz Haaz et al., 2024; PMID: 39222336). The analysis demonstrated that while corticosteroid injections provide rapid short-term pain relief, their benefits rapidly decline after 4 to 6 weeks. In contrast, PRP injections demonstrated superior and sustained improvements in both pain (Visual Analog Scale) and physical function (WOMAC scores) at 6 and 12 months. The study concluded that PRP offers superior long-term clinical efficacy and is highly effective at preserving joint structures compared to corticosteroids.
Furthermore, concerns regarding the safety profile of PRP compared to steroids have been clarified. A large-scale meta-analysis of randomized controlled trials published in Arthroscopy evaluated the complication rates of joint injections (Complications of Platelet-Rich Plasma Injection, 2025; PMID: 40409439). The study analyzed safety data across thousands of patients and concluded that the overall complication rate of PRP is exceptionally low and no different from that of standard corticosteroids or hyaluronic acid gel injections. The primary side effects are limited to mild, temporary local pain and stiffness associated with the initial post-injection inflammatory flare, confirming that PRP is a highly safe, biocompatible treatment.
Head-to-Head Comparison: Steroids vs. Platelet-Rich Plasma (PRP)
To help patients make an informed decision, the table below compares the clinical parameters of corticosteroids and Platelet-Rich Plasma (PRP) injections based on current medical literature:
| Parameter | Corticosteroids (Steroids) | Platelet-Rich Plasma (PRP) |
|---|---|---|
| Primary Mechanism | Chemical suppression of inflammation | Direct delivery of active growth factors to trigger repair |
| Onset of Relief | Rapid (24 to 48 hours) | Gradual (4 to 6 weeks) |
| Duration of Benefit | Short-term (4 to 12 weeks) | Long-term (12+ months) |
| Impact on Cartilage | Chondrotoxic (accelerates volume loss) | Chondroprotective (stimulates matrix synthesis) |
| Typical Sessions | Single injection (limited to 3/year in same joint) | 1 to 3 injections (spaced 2–4 weeks apart) |
| Biological Source | Synthetic chemical pharmaceutical | Autologous (patient's own blood platelets) |
Dynamic Ultrasound Guidance: Target Accuracy for Joint Injections
Regardless of whether we are injecting steroids or PRP, the clinical outcome depends entirely on injection accuracy. Historically, doctors performed joint injections using "blind" or landmark-guided techniques—meaning they felt the bone structures and inserted the needle based on anatomic estimation. However, research shows that up to 20% to 30% of blind knee injections, and up to 40% of blind shoulder injections, miss the intended target space, depositing the therapeutic fluid into surrounding fat pads or muscle tissue where it cannot promote healing or may cause adverse tissue degradation.
To prevent this, my clinic utilizes high-resolution musculoskeletal ultrasound for every procedure. In clinical diagnostics, Musculoskeletal ultrasound (MSKUS) is a point-of-care imaging modality that utilizes high-frequency sound waves to visualize tendons, ligaments, muscles, nerves, and joint spaces in real-time. By utilizing MSKUS, we can trace the needle tip dynamically as it enters the skin, passes through the tissues, and enters the exact target zone. For PRP, we can guide the needle directly into the joint recess, the tendon sheath, or the precise margins of a cartilage defect or meniscus tear, ensuring 100% target accuracy and maximizing the healing effect.
Clinical Decision Framework: Which Injection Do You Need?
Choosing the right injection is a clinical decision that must be personalized based on the patient's specific tissue state, degree of joint wear, and functional goals. Below is the diagnostic decision framework I utilize in my practice:
- The Cortisone Route (When to use steroids): I recommend a corticosteroid injection when a patient presents with an acute, severe inflammatory crisis. For example, a patient with a massive gouty flare-up or acute knee bursitis who cannot walk or sleep due to excruciating pain. In these severe, mobility-limiting scenarios, immediate pain relief is the priority. However, this is used as a short-term bridge (limited to 1 or 2 injections) to quiet the joint before transitioning to structural therapies or progressive rehabilitation.
- The PRP Route (When to use PRP): PRP is the gold standard for patients with active soft-tissue tears (such as partial rotator cuff tears or meniscus tears), moderate-to-severe joint osteoarthritis, or chronic tendinopathies that have failed to heal with conservative management. PRP is chosen when we require a high concentration of growth factors to actively stimulate cartilage chondrocytes and regulate the joint environment.
It is critical to establish realistic clinical expectations. PRP injections are not quick fixes. Because they rely on biological tissue repair, patients must follow a structured, progressive loading physical therapy program. We start with gentle isometric exercises to maintain joint motion, gradually progressing to eccentric and isotonic loading to guide the alignment of newly deposited collagen fibers in the tendons and ligaments (litid) surrounding the joint.
Practical Barriers & Care Adaptations for Northern Luzon Patients
When designing a care plan for patients in Northern Luzon, we must address the real-world practical barriers they face. Many of my patients travel from distant municipalities in Ilocos Sur, Ilocos Norte, or Abra to reach our clinic in Vigan. Traveling several hours on public transport or rough roads with a painful, unstable joint is a major challenge. For these patients, scheduling frequent weekly visits is unrealistic. To minimize travel burden, we structure our PRP sessions with wider spacing (4 to 6 weeks apart) and provide comprehensive, structured home-based exercise protocols so they can perform their rehabilitation safely without requiring daily travel to a physical therapy clinic.
Furthermore, financial constraints are a primary factor in healthcare decisions in the Philippines. Traditional HMOs and PhilHealth do not cover premium regenerative therapies like PRP, requiring patients to pay out-of-pocket. To address this, we maintain complete transparency in our pricing models. We explain that while a steroid shot is inexpensive upfront, its temporary nature leads to a repetitive cycle of injections and escalating cartilage damage, eventually resulting in the need for a total joint replacement surgery. A joint replacement in the Philippines is a massive financial burden, costing hundreds of thousands of pesos in hospital bills, orthopedic implants, anesthesia, and months of post-operative care. In contrast, a structured series of PRP injections preserves the patient's natural joint, prevents surgery, and is highly cost-efficient over the long term.
We also respect local cultural preferences. In Ilocos, many patients initially seek relief through traditional massage or hilot. While gentle rubbing can temporarily soothe aching muscles, it cannot repair a torn ligament or reverse cartilage wear. I counsel my patients that they do not need to abandon their trust in traditional comfort, but they must complement it with objective, ultrasound-guided medical interventions to restore the structural integrity of their joints and ensure safe, long-term mobility.
Schedule Your Consultation in Vigan City
If you are tired of temporary pain relief and want to explore if Platelet-Rich Plasma (PRP) is the right treatment for your joint pain, you can schedule a comprehensive evaluation at our clinic. Contact our team today to book your appointment and consultation with Dr. Ben Paolo C. Rabara to reserve a slot.
References & Clinical Evidence
- [1] McAlindon TE, et al. Effect of Intra-articular Triamcinolone vs Saline on Knee Cartilage Volume and Pain in Patients With Knee Osteoarthritis: A Randomized Clinical Trial. JAMA. 2017 May 16;317(19):1961-1969. doi: 10.1001/jama.2017.5283. PMID: 28510679.
- [2] Diaz Haaz J, et al. Corticosteroid injections for knee osteoarthritis offer clinical benefits similar to hyaluronic acid and lower than platelet-rich plasma: a systematic review and meta-analysis. EOR. 2024 Sep 2;9(9):603-614. doi: 10.1530/EOR-24-0045. PMID: 39222336.
- [3] Complications of Platelet-Rich Plasma Injection for Knee Osteoarthritis Are Similar to Those of Corticosteroids and Hyaluronic Acid but Are Significantly Greater Than Those of Placebo Injections: A Meta-analysis of Randomized Controlled Trials. Arthroscopy. 2025 Jan;41(1):288-298. doi: 10.1016/j.arthro.2024.06.012. PMID: 40409439.
- [4] Tendon Ruptures Associated With Corticosteroid Therapy. PMCID: PMC1237870. PMID: 919538.
* Clinical references are provided to support the medical claims made in this article. TeraCare adheres to evidence-based practices in physical medicine and rehabilitation.

Dr. Ben Rabara
Dr. Ben Rabara is a Board-Certified Physiatrist specializing in Physical Medicine and Rehabilitation. He focuses on non-surgical, precision treatments for musculoskeletal conditions, utilizing advanced diagnostics like MSK Ultrasound.
Medical Disclaimer: The information provided in this article is for educational purposes only and does not substitute for professional medical advice, diagnosis, or treatment. Always consult a qualified physician for your specific health conditions.